








LARYNX
LARYNGOLOGY

LARYNGOLOGY is an area of Otorhinolaryngology that studies diseases of the larynx and the voice.
The voice is an important communication tool and through this we also express our feelings and desires.
The voice is produced in the larynx, during the expiration of air between the vocal folds (vocal chords), modified by the structure called the vocal tract, which defines the personality of our voices.
Vocal expression can then reveal a little about ourselves or even express signs about the health of our body. A change in voice production is called dsyphonia, and can manifest in different ways, such as: hoarseness, vocal tiredness, pain when speaking, difficulty to maintain or achieve notes among others.
Any change in the voice that lasts more than 15 days should be investigated.
There are many possible causes for voice changes, and it should be evaluated depending on age groups and even different professional activities. Voice professionals, who include teachers, singers, and telemarketing operators, are more likely to be affected by vocal changes due to more intensive use of the voice, and these changes can be divided between abuse and bad use of the voice. With vocal abuse, we use the voice above recommended limits and with bad vocal usage, we see compromises in primary voice production.
Different age groups need careful approach, due to the fact that some pathology will appear more in some ages, resulting in differentiated use of the voice. In children, for example, bad use of the voice resulting from inadequate vocal behavior, like those who shout a lot, increase the incidence of the vocal nodules (calluses). Already in more advanced age groups, the physiopathological consequences of this condition cause phonatory compromise, mainly with loss of vocal potential.
Environmental factors, pollutants and addictions such as nicotine and frequent consumption of alcoholic beverages increases the incidence of different pathologies in the vocal tract a lot, in particular the larynx, with repercussions in pronunciation and even breathing. Nowadays the World Health Organization (WHO) observes a high incidence of neoplasm in the respiratory tract and pronunciation, with the recommendation for a systematic investigation, whenever the symptoms persist.
National and international campaigns, in particular the campaigns during Voice Week and World Voice Day (16th April), has alerted the population of our country with regards to caring for their voice.
THE LARYNX
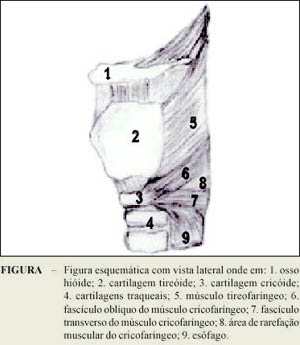
The larynx is located in the neck region and located by the pharynx and plays an important part in swallowing and in phonation.
It has cartilage in its structure and internally possesses 5 pairs of small muscles, called intrinsics, which perform the function producing and modulating the voice. Internally it is covered by the respiratory mucous membrane, with the exception of the region between the vocal folds, where epithelium (the covering) is stratified squamous.
For voice production the larynx receives neural stimulus, which permits a controlled approach of the vocal folds (adduction) that modulates the passage of the air exhaled, in this way producing a sound between the vocal folds. This sound will be amplified and modified by the upper airway, which consists of the vocal tract. When we breathe the vocal folds separate (abduction), which permits the opening of the area in the region of the glottis. In this way each one of us has diverse vocal identities, resulting from the differences in our vocal tracts.
Differences between the sexes are noticeable, as much anatomical as functional, giving the difference in the quality of the voice between men and women. Women produce an average fundamental frequency in the 200 Hz and men in the 100 Hz.
The larynx has an important role in swallowing, as much as having to reconfigure the airway between respiratory and digestive systems, as in the protection of the entrance of the airway, due to sensory innervation of the glottis and super-glottis region.
The execution of endoscopic procedures is painless and relatively simple under local anesthesia (lidocaine spray), in an ambulatory setting and of quick duration. Normally soon after the endoscopic examination a report is provided, containing descriptive information about the examination. When necessary or requested by the patient, without doctor’s assistant or speech therapist, these examinations can be recorded on videotape tapes or DVD.
For children as part of the investigation of possible pathologies of the upper airways, the procedure used is a video nasopharyngolaryngoscopy, which is performed in the environment of the surgical center, under an inhaled anesthesia (gas inhalant). With this treatment, today we are able to examine children of all age groups, in safety and comfort, which permits a precise diagnosis.
DIAGNOSIS
The Otorhinolaryngologic evaluation (ORL) is of fundamental importance for the diagnosis of diseases that can affect the voice.
Everything begins with a detailed interview, with information about the quality of the vocal complaint, duration of the symptoms, evolution, prior treatment, investigation of associated causes, identification of irritants of the airways, type of professional activity etc.
After general otorhinolaryngologic evaluation, the detailed investigation (by means of examinations) is the next step. In recent years there has been a spectacular advancement in the quality of medical instruments, facilitating the diagnosis of diseases of the larynx.
When treating the airways, we can use a combination of materials, which at the same time allow an objective, detailed and precise investigation, permitting not just lesional diagnosis but also functional.
We are able to perform LARYNGOSCOPY, with telescopic or fiber optic, both being coupled to a video system, which allows the participation of the patient in his examination, facilitating understanding of the diagnosis.
most COMMON dieseases of THE LARYNX
LARYNGITIS
Any inflammatory activity that affects the region of the larynx and its surroundings is considered as laryngitis. The most common cause of laryngitis is viral infections. Haemophilus influenza is the agent most frequently related to viral processes, which may only manifest in the larynx or may be related to the airways as a whole. The most frequent clinical manifestation is dsyphonia, mainly hoarseness; however it can be associated with throat pain or a cough. Bacterial processes can also cause laryngitis, however these are generally a result of complications from viral laryngitis or will be related to the lower airways. A fungal infection is frequently linked to low general or local immunity, and can be found, for example, in patients being treated for bronchial asthma with corticosteroid sprays.
Finally the most frequent cause is the laryngitis caused by Gastroesophageal Reflux. As well as a varied range of symptoms, such as dsyphonia, cough, frog in the throat and sensation of a ball "caught "in the throat, it can also be related to several lesions in the mucous membrane of the larynx, in particular in the posterior region, as it is this region that is in close proximity to the esophagus.
VOCAL NODULES
Vocal nodules are the most frequent lesions with voice professionals, which include teachers, singers, radio announcers, priests etc.
They are generally formed by phonatory trauma resulting from conditions of abuse or bad use of the voice. As a characteristic, the vocal nodules are present in both the vocal folds. They are still the most common injury of children with hoarseness.
The bigger the vocal nodules, the bigger the glottal gap that appears with the contact between the vocal folds in phonation, and the bigger the gap, the bigger the escape of air, which determines the progressive degrees of dysphonia.
They are benign lesions, with a large possibility of reabsorption with conservative treatment, mainly Speech Therapy.

VOCAL POLYPS AND REINKE’S EDEMA
Polyps of the larynx are inflammatory, benign lesions, also associated to phonatory trauma, however here we find others factors associated, such as inflammation of the upper airways, nicotine addiction, reflux and as a consequence of pre-existing wounds in the vocal folds.
There are a lot of variables, as they can be small, big, wide or pediculated, clear, jellylike or hemorrhagic, united or bilateral. The phonatory impact is a more variable, as it is always bigger than with vocal nodules. The majority of cases require treatment with endoscopic microsurgery.
With Reinke’s Edema, we find a diffuse jellylike edema that takes up the extent of the vocal folds, and generally is bilateral. Attacks with more frequent in middle-aged women and smokers. The vocal quality drops, becoming more severe and even can cause a certain degree of respiratory discomfort when they are big.

INTRA-CHORDAL CYSTS and VOCAL FURROWS
They are lesions of the larynx classified as minimal structural changes, together with other three lesions, such as the micro-diaphragm of the anterior commissure, the vascular dysgenesis and the bridge of the mucous membrane.
They are congenital lesions that cause a big phonatory impact, due to the fact they are located in the deepest layers of the vocal folds, therefore affecting functionality of voice production and usually demanding microsurgical treatment.
The cysts can be open or closed and the furrows also occur in different forms, depending on the degree of penetration of the furrow into the vocal folds.
Intra-chordal cysts should be differentiated from pseudocysts due to the location of its formation in the superficial layer (epithelial) of the vocal folds.
LEUCOPLASY
Leucoplasy are lesions produced by continued, intense and chronic irritation of the mucous covering the vocal folds, mainly in the more superficial layer. They are lesions that are white in color and different degrees of thickness. They are considered as pre-malignant lesions and, therefore their treatment and monitoring should be done with care, as they can evolve into cancer of the Larynx.

PARALYSIS
The larynx is covered by motor and sensory innervations, the vagus nerve, through its branches: superior and inferior laryngeal nerves. The inferior laryngeal nerve is also known as the recurrent nerve and gives most of the motor innervation to the intrinsic muscles of the larynx. Therefore in the majority of unilateral paralysis, there is a recurring problem with the laryngeal nerve.
As the vocal fold becomes paralyzed, unilaterally or bilaterally, before starting any therapy, possible causes should be investigated, as the area of innervation is very comprehensive and these causes can be from the brain, the brain stem, neck and even the chest.
Depending on the kind of the paralysis, of the position of the paralyzed vocal fold, different treatment can be appropriate, such as speech therapy, endoscopic surgery and, neck surgeries like Thyroplasty, to move the paralyzed vocal fold to the middle, thus restoring vocal quality.
LARYNGEAL PAPILLOMATOSIS
This disease is very common, and affects children and adults, with greater frequency in children. Because of this two forms have evolved, Juvenile Papillomatosis, in general more serious and Adult Papillomatosis.
Papillomatosis is a benign lesio9n, of viral origin from the group of HPV viruses; however other sub-types can be acquired (birth canal, blood, sexual relations) or transmitted to the child via the placenta of the mother. They are located in the mucous membrane of pharynx and characteristically in the larynx, forming a tumoural outgrowth.
It is known to be the most common benign tumor in the larynx, however it should be stated once again that its origin is viral. It causes gradual changes to the voice that can evolve into Aphony (total voice lose) and in more advanced cases cause obstruction of the airways at the glottis level. Precise diagnosis allows curative treatment of this illness.

NEOPLASM
Malignant neoplasms in the larynx are common and caused mainly by harmful agents to the mucous membrane of the airways, such as smoking and frequent consumption of alcoholic beverages. National campaigns for vocal health have alerted the public to these risks, allowing for greater detection at the early stages, permitting treatment with a curative result. More than 90% of neoplasms of the larynx are represented by Epidermoid Carcinoma. These lesions can initially manifest with dysphonia, but very big and advanced lesions can cause difficulty with breathing (dyspnea). The earlier the diagnosis, the better the result of treatment, with restoration of the phonatory functions.
The bigger the wounds, the bigger the risk for open surgery of the larynx for partial or even total removal of the diseased structure. In cases of total Laryngectomy, the possibility of development by means of training esophageal speech or the implementation of the Bloom-Singer speech valve allow for speech recuperation even though it is in a limited way.

treatnent for diseases OF THE VOICE AND LARyNGOLoGICal WOUNDS
MEDICAMENTAL TREATMENT:
Medicamental treatment will be prescribed whenever there are signs and symptoms of inflammation in the pharynx or larynx and will depend on the causal pathology and of the stage of evolution. Other medicamental treatments of the larynx can include inter-lesional injections such as in cases of Papillomatosis of the larynx, when we apply an unspecific anti-viral medicine (cidofovir) endoscopically
For the treatment of the spasmodic dsyphonia, we apply Botulinum Toxin, along with electromyography of the larynx (LEMG).
SPEECH THERAPY TREATMENT
The participation of a professional speech therapist in Laryngology is of fundamental importance, as this professional will frequently participate in the care of phonatory problems, as much the treatment as the prevention of vocal problems, such as rehabilitation exercise for the treatment of lesions and post-operative orientation.
Their participation will still be desired for post-therapy monitoring and also in many other ways, for example, in the new field of vocal esthetics indicated to prepare voice professionals for better results and performance in their functions.
The treatment techniques, duration of treatment and follow up, are specified, case by case, depending on the needs of each clinical case.
SURGICAL TREATMENT
Diseases of the larynx that cannot be resolved just with medicamental treatment, or do not respond to speech therapy, could be submitted for surgical treatment, depending on others factors, such as: base pathology, clinical evolution, physical condition of the patient and degree of functional compromise.
Benign lesions invariably are treated surgically using microsurgery of the larynx. As the name suggests, it is an endoscopic technique, using an optical microscope. It is a delicate technique, being part of the minimal invasive procedures.
This procedure is performed in the surgical center, under general anesthesia, as the region of the larynx as well as being located internally and distal in the neck, is still very sensitive and cause many reflexes.
These procedures are of short duration and the patient is normally discharged on the same day of the procedure, with post-surgical orientation, one of them being that there is no restriction regarding post-operative eating.
Many different techniques exist that will be applied during microsurgery, after the placement of the surgical laryngoscope and linkage of the microscopy system. These techniques will be chosen depending on the lesions to be operated, of their dimensions and location in the larynx. The procedure is painless and for the period of post-operative recuperation, vocal rest is recommended for a week, when speech therapy will be started.
Other surgical treatments can also be used for the larynx, among them being medialization of the larynx in cases of paralysis of the vocal folds.
The treatment of cancer of the larynx is also performed endoscopically, when in initial stages; however other techniques can be applied for more advanced cases.